Building upon our previous research conducted at weekly and monthly intervals, this study investigates the yearly dynamics of weather conditions and air quality on respiratory diseases, specifically tailored to Faial Island in the Azores. Expanding our analysis to a yearly basis allows for a more comprehensive understanding of long-term trends and seasonal variations in hospital admissions. Drawing upon extensive daily data spanning from 2008 to 2019, sourced from the Statistics Service of Hospital da Horta, the Meteorological Observatory Príncipe Alberto de Mónaco, and the Air Quality Monitoring Network of the Azores, we examined the differentiated relationships between yearly meteorological variables, such as temperature, dew point, and wind direction, and respiratory health outcomes. Additionally, we explored the persistent influence of air quality indicators, including suspended particulate matter with an aerodynamic diameter of 10 micrometers (µm) or less (PM10), sulfur dioxide (SO2), nitrogen dioxide (NO2), and ozone (O3), across different seasons and years. By incorporating yearly data into our analysis, this study aims to provide a comprehensive and nuanced understanding of the interplay between environmental factors and respiratory disease hospitalizations, thereby informing targeted interventions and public health strategies in insular regions. The principal component analysis (PCA) applied to the yearly data reveals interesting correlation patterns between meteorological variables and hospitalizations for respiratory diseases such as asthma, pneumonia, and rhinitis. Hospital admissions were found to increase during periods of lower temperatures and smaller temperature amplitudes, suggesting that prolonged cold conditions may exacerbate symptoms of these diseases. Additionally, atmospheric pollutant concentrations, such as suspended particles PM10, SO2, NO2, and O3, significantly varied across seasons, with a notable influence on the exacerbation of respiratory diseases. In insular regions like the Azores, these findings highlight the importance of targeted public health strategies to mitigate the impact of environmental factors on respiratory health.
| Published in | American Journal of Health Research (Volume 12, Issue 6) |
| DOI | 10.11648/j.ajhr.20241206.12 |
| Page(s) | 165-178 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Respiratory Diseases, Hospital Admissions, Meteorological Parameters, Air Quality, Azores Region
FF | Wind Speed |
HR | Relative Humidity |
NO2 | Nitrogen Dioxide |
O3 | Ozone |
PCA | Principal Component Analysis |
PM10 | Particulate Matter with a Diameter of 10 Micrometers or Less |
Pnmm | Mean Sea Level Pressure |
RDH | Respiratory Diseases Hospitalizations |
RR | Total Precipitation |
SO2 | Sulfur Dioxide |
Tam | Mean Air Temperature |
TD | Dew Point Temperature |
Tmn | Minimum Air Temperature |
Tmx | Maximum Air Temperature |
Tha | Air Termal Amplitude |
| [1] | Zarocostas, J (2023) WMO calls for greater use of climate services in health. The Lancet, Volume 402, Issue 10414, 1737. |
| [2] | Darnell MER, Subbarao K, Feinstone SM, Taylor DR (2004) Inactivation of the coronavirus that induces severe acute respiratory syndrome, SARS-CoV. J Virol Methods 121: 85–91. |
| [3] | Abe T, Tokuda Y, Ohde S, et al (2009) The relationship of short-term air pollution and weather to ED visits for asthma in Japan. American Journal of Emergency Medicine 27: 153–159. |
| [4] | Li M, Li Q, Yang G, et al (2011) Cold temperature induces mucin hypersecretion from normal human bronchial epithelial cells in vitro through a transient receptor potential melastatin 8 (TRPM8)-mediated mechanism. Journal of Allergy and Clinical Immunology 128. |
| [5] | Douglas – Vail M, Jiang A, Erdelyi S, Brubacher JR, Abu-Laban RB. (2023). Association of air quality during forest fire season with respiratory emergency department visits in Vancouver, British Columbia. The Journal of Climate Change and Health, Volume 13, 100255, ISSN 2667-2782, |
| [6] | Kangas T, Gadayne S, Lefebre, W, Vanpoucke C, Rodriguez-Loureiro L (2023). Are air quality perception and PM2.5 exposure differently associated with cardiovascular and respiratory disease mortality in Brussels? Findings from a census-based study. Environmental Research 219 (2023) 115180. |
| [7] | Anderson, J. O., Thundiyil, J. G. & Stolbach, A. Clearing the Air: A Review of the Effects of Particulate Matter Air Pollution on Human Health. J. Med. Toxicol. 8, 166–175 (2012). |
| [8] | Pranata R, Huang I, Lim MA, Wahjoepramono EJ, July J. Impact of cerebrovascular and cardiovascular diseases on mortality and severity of COVID-19-systematic review, meta-analysis, and meta-regression. J Stroke Cerebrovasc Dis. 2020 Aug; 29(8): 104949. Epub 2020 May 14. PMID: 32410807; PMCID: PMC7221373. |
| [9] | Nieuwenhuijsen MJ, Basagaña X, Dadvand P, Martinez D, Cirach M, Beelen R, Jacquemin B, (2014). Air pollution and human fertility rates, Environment International, Volume 70, Pages 9-14, ISSN 0160-4120, |
| [10] | Chen J, Hoek G. Long-term exposure to PM and all-cause and cause-specific mortality: A systematic review and meta-analysis. Environ Int. 2020 Oct; 143: 105974. Epub 2020 Jul 20. PMID: 32703584. |
| [11] | Hoek, G., Krishnan, R. M., Beelen, R. et al. Long-term air pollution exposure and cardio- respiratory mortality: a review. Environ Health 12, 43 (2013). |
| [12] | Hvidtfeldt UA, Sørensen M, Geels C, Ketzel M, Khan J, Tjønneland A, Overvad K, Brandt J, Raaschou-Nielsen O. Long-term residential exposure to PM2.5, PM10, black carbon, NO2, and ozone and mortality in a Danish cohort. Environ Int. 2019 Feb; 123: 265-272. Epub 2018 Dec 12. PMID: 30551059. |
| [13] | Mireku N, Wang Y, Ager J, Reddy RC, Baptist AP. Changes in weather and the effects on pediatric asthma exacerbations. Ann Allergy Asthma Immunol. 2009 Sep; 103(3): 220-4. PMID: 19788019. |
| [14] | Marno P, Bryden C, Bird W, Watkin HA (2006) How different measures of cold weather affect chronic obstructive pulmonary disease (COPD) hospital admissions in London. European Respiratory Review 15: 185–186. |
| [15] | Koskela HO (2017) Cold air-provoked respiratory symptoms: the mechanisms and management Cold Air-Provoked Res-piratory Symptoms: The Mechanisms and Management. 3982. |
| [16] | Michelozzi P, Accetta G, De Sario M, et al (2009) High Temperature and Hospitalizations for Cardiovascular and Respiratory Causes in 12 European Cities. Am J Respir Crit Care Med 179: 383–389. |
| [17] | Strickland MJ, Darrow LA, Klein M, et al (2010) Short-term Associations between Ambient Air Pollutants and Pediatric Asthma Emergency Department Visits. Am J Respir Crit Care Med 182: 307–316. |
| [18] | Zhang Y, Peng L, Kan H, et al (2014) Effects of meteorological factors on daily hospital admissions for asthma in adults: A time-series analysis. PLoS One 9: |
| [19] | Fitzgerald EF, Pantea C, Lin S (2014) Cold Spells and the Risk of Hospitalization for Asthma: New York, USA 1991–2006. Lung 192: 947–954. |
| [20] | Bodaghkhani E, Mahdavian M, Maclellan C, et al (2019) Effects of meteorological factors on hospitalizations in adult patients with asthma: A systematic review. Can Respir J 2019: |
| [21] | Dharmage SC, Perret JL, Custovic A (2019) Epidemiology of asthma in children and adults. Front Pediatr 7. |
| [22] | To T, Stanojevic S, Moores G, et al (2012) Global asthma prevalence in adults: Findings from the cross-sectional world health survey. BMC Public Health 12: 204. |
| [23] | Koper I, Hufnagl K, Ehmann R (2017) Gender aspects and influence of hormones on bronchial asthma - Secondary publication and update. World Allergy Organization Journal 10: 1–7. |
| [24] | Caetano, M., Santos, A., Carvalho, B., Cordeiro, C., Barreto, C., Gomes, E., Barata, F., Félix, F., Queiroga, H., Bernardo, J., Cardoso, J., Bandera, T., Brito, U., Hespanhol, V (2015). Pneumologia. Rede Nacional de Especialidade Hospitalar e de Refe-renciação. Ministério da Saúde. Governo de Portugal. Lisboa. |
| [25] | Sousa C, Soares A, Morais L, Silva R (2019) Indicadores de Saúde 2013 - 2018, Região Autónoma dos Açores. Angra do Heroismo. |
| [26] | Carvalho F, Martins D, Meirelles M, Vasconcelos H (2022a) Weather and Air Quality Factors Contribution to the Hospital Admissions of Patients with Respiratory Diseases : Case Study of Faial Island (Azores). 31: |
| [27] | Arias PA, Bellouin N, Coppola E, et al (2021) Technical Summary. In: Masson-Delmotte V, P. Zhai PA, Connors SL, et al. (eds) Climate Change 2021: The Physical Science Basis. Contribution of Working Group I to the Sixth Assessment Report of the Intergovernmental Panel on Climate Change |
| [28] | Carvalho F, Meirelles M, Henriques D, et al (2022b) Climate Change and the Increase of Extreme Events in Azores. In: Leal Filho W (ed) Handbook of Human and Planetary Health. Climate Change Management. Springer, |
| [29] | Hernández A, Kutiel H, Trigo RM, Valente MA, Sigró J, Cropper T, Santo FE 2016). New Azores archipelago daily precipi-tation dataset and its links with large-scale modes of climate variability. Int. J. Climatol., 36 (2016), pp. 4439-4454, |
| [30] | Huan Minh Tran, Feng-Jen Tsai, Yueh-Lun Lee, Jer-Hwa Chang, Li-Te Chang, Ta-Yuan Chang, Kian Fan Chung, Han-Pin Kuo, Kang-Yun Lee, Kai-Jen Chuang, Hsiao-Chi Chuang (2023). The impact of air pollution on respiratory diseases in an era of climate change: A review of the current evidence. Science of The Total Environment, Volume 898, 166340, ISSN 0048-9697. |
| [31] | Anjeni Keswani, Hana Akselrod, Anenberg Susan C. Health and clinical impacts of air pollution and linkages with climate change. NEJM Evidence 2022; 1: EVI Dra2200068. |
| [32] | Lewis J. Z. Weeda, Corey J. A. Bradshaw, Melinda A. Judge, Chitra M. Saraswati, Peter N. Le Souëf (2024). How climate change degrades child health: A systematic review and meta-analysis. Science of The Total Environment, Volume 920, 170944, ISSN 0048-9697. |
| [33] | Landsberg HE (1972) The Assessment of Human Bioclimate - a limited review of physical parameters. World Meteorological Organization TECHNICAL: 1–36. |
| [34] | Damini Singh, Indrani Gupta, Arjun Roy (2023). The association of asthma and air pollution: Evidence from India. Economics & Human Biology, Volume 51, 101278, ISSN 1570-677X. |
APA Style
Carvalho, F., Meirelles, M., Martins, D., Vasconcelos, H. C. (2024). Yearly Assessment of Weather and Air Quality Impact on Respiratory Disease Hospitalizations: Faial Island (Azores) Study. American Journal of Health Research, 12(6), 165-178. https://doi.org/10.11648/j.ajhr.20241206.12
ACS Style
Carvalho, F.; Meirelles, M.; Martins, D.; Vasconcelos, H. C. Yearly Assessment of Weather and Air Quality Impact on Respiratory Disease Hospitalizations: Faial Island (Azores) Study. Am. J. Health Res. 2024, 12(6), 165-178. doi: 10.11648/j.ajhr.20241206.12
AMA Style
Carvalho F, Meirelles M, Martins D, Vasconcelos HC. Yearly Assessment of Weather and Air Quality Impact on Respiratory Disease Hospitalizations: Faial Island (Azores) Study. Am J Health Res. 2024;12(6):165-178. doi: 10.11648/j.ajhr.20241206.12
@article{10.11648/j.ajhr.20241206.12,
author = {Fernanda Carvalho and Maria Meirelles and Daniela Martins and Helena Cristina Vasconcelos},
title = {Yearly Assessment of Weather and Air Quality Impact on Respiratory Disease Hospitalizations: Faial Island (Azores) Study
},
journal = {American Journal of Health Research},
volume = {12},
number = {6},
pages = {165-178},
doi = {10.11648/j.ajhr.20241206.12},
url = {https://doi.org/10.11648/j.ajhr.20241206.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajhr.20241206.12},
abstract = {Building upon our previous research conducted at weekly and monthly intervals, this study investigates the yearly dynamics of weather conditions and air quality on respiratory diseases, specifically tailored to Faial Island in the Azores. Expanding our analysis to a yearly basis allows for a more comprehensive understanding of long-term trends and seasonal variations in hospital admissions. Drawing upon extensive daily data spanning from 2008 to 2019, sourced from the Statistics Service of Hospital da Horta, the Meteorological Observatory Príncipe Alberto de Mónaco, and the Air Quality Monitoring Network of the Azores, we examined the differentiated relationships between yearly meteorological variables, such as temperature, dew point, and wind direction, and respiratory health outcomes. Additionally, we explored the persistent influence of air quality indicators, including suspended particulate matter with an aerodynamic diameter of 10 micrometers (µm) or less (PM10), sulfur dioxide (SO2), nitrogen dioxide (NO2), and ozone (O3), across different seasons and years. By incorporating yearly data into our analysis, this study aims to provide a comprehensive and nuanced understanding of the interplay between environmental factors and respiratory disease hospitalizations, thereby informing targeted interventions and public health strategies in insular regions. The principal component analysis (PCA) applied to the yearly data reveals interesting correlation patterns between meteorological variables and hospitalizations for respiratory diseases such as asthma, pneumonia, and rhinitis. Hospital admissions were found to increase during periods of lower temperatures and smaller temperature amplitudes, suggesting that prolonged cold conditions may exacerbate symptoms of these diseases. Additionally, atmospheric pollutant concentrations, such as suspended particles PM10, SO2, NO2, and O3, significantly varied across seasons, with a notable influence on the exacerbation of respiratory diseases. In insular regions like the Azores, these findings highlight the importance of targeted public health strategies to mitigate the impact of environmental factors on respiratory health.
},
year = {2024}
}
TY - JOUR T1 - Yearly Assessment of Weather and Air Quality Impact on Respiratory Disease Hospitalizations: Faial Island (Azores) Study AU - Fernanda Carvalho AU - Maria Meirelles AU - Daniela Martins AU - Helena Cristina Vasconcelos Y1 - 2024/11/18 PY - 2024 N1 - https://doi.org/10.11648/j.ajhr.20241206.12 DO - 10.11648/j.ajhr.20241206.12 T2 - American Journal of Health Research JF - American Journal of Health Research JO - American Journal of Health Research SP - 165 EP - 178 PB - Science Publishing Group SN - 2330-8796 UR - https://doi.org/10.11648/j.ajhr.20241206.12 AB - Building upon our previous research conducted at weekly and monthly intervals, this study investigates the yearly dynamics of weather conditions and air quality on respiratory diseases, specifically tailored to Faial Island in the Azores. Expanding our analysis to a yearly basis allows for a more comprehensive understanding of long-term trends and seasonal variations in hospital admissions. Drawing upon extensive daily data spanning from 2008 to 2019, sourced from the Statistics Service of Hospital da Horta, the Meteorological Observatory Príncipe Alberto de Mónaco, and the Air Quality Monitoring Network of the Azores, we examined the differentiated relationships between yearly meteorological variables, such as temperature, dew point, and wind direction, and respiratory health outcomes. Additionally, we explored the persistent influence of air quality indicators, including suspended particulate matter with an aerodynamic diameter of 10 micrometers (µm) or less (PM10), sulfur dioxide (SO2), nitrogen dioxide (NO2), and ozone (O3), across different seasons and years. By incorporating yearly data into our analysis, this study aims to provide a comprehensive and nuanced understanding of the interplay between environmental factors and respiratory disease hospitalizations, thereby informing targeted interventions and public health strategies in insular regions. The principal component analysis (PCA) applied to the yearly data reveals interesting correlation patterns between meteorological variables and hospitalizations for respiratory diseases such as asthma, pneumonia, and rhinitis. Hospital admissions were found to increase during periods of lower temperatures and smaller temperature amplitudes, suggesting that prolonged cold conditions may exacerbate symptoms of these diseases. Additionally, atmospheric pollutant concentrations, such as suspended particles PM10, SO2, NO2, and O3, significantly varied across seasons, with a notable influence on the exacerbation of respiratory diseases. In insular regions like the Azores, these findings highlight the importance of targeted public health strategies to mitigate the impact of environmental factors on respiratory health. VL - 12 IS - 6 ER -
Portuguese Institute for Sea and Atmosphere (IPMA), Ponta Delgada, Portugal
Biography: Fernanda Carvalho is a graduate in Physics – Atmospheric Physics from the University of Aveiro (1988) and holds a master’s degree in Geophysical Sciences – Meteorology from the University of Lisbon (1998). She has extensive experience in meteorology, particularly in atmospheric observation, forecasting, and radiation studies. She joined the National Institute of Meteorology and Geophysics as a senior meteorologist in 1992 and led the implementation of the UV Index Forecasting Program in Portugal from 1999. She coordinated the Azores Weather Forecasting and Surveillance Center (2015-2019) and currently works at the Portuguese Institute for Sea and Atmosphere. She has contributed to numerous scientific publications and research projects, and lectures at the University of the Azores.

Faculty of Science and Technology, University of the Azores, Ponta Delgada, Portugal; Research Institute of Marine Sciences, University of the Azores, Faial, Portugal
Biography: Maria Meirelles has a Diploma in Physics from the State University of Rio de Janeiro, Brasil in 1992, a Geophysics Master in the field of Meteorology from University of Lisbon (Faculty of Sciences), Portugal in 1997 and got her PhD in Physics from the Azores University (UAC), Portugal in 2009, in the field of Geophysical Sciences. Her teaching activities include topics on meteorology/atmosphere/climatology, general physics, physics for biology and geophysics, among others, for undergraduate and master studies. She has participated in several scientific conferences, and she has published several research articles.

Faculty of Science and Technology, University of the Azores, Ponta Delgada, Portugal
Biography: Daniela Martins holds a degree in Biology and a Master’s in Environment, Heath and Security from the University of the Azores. She is currently conducting research on the impact of weather and air quality on respiratory disease hospitalizations. Her work[ focuses on analysing how meteorological variables and air pollutants affect respiratory health, contributing to the understanding and mitigation of risks associated with adverse environmental conditions.

Faculty of Science and Technology, University of the Azores, Ponta Delgada, Portugal; Laboratory of Instrumentation, Biomedical Engineering and Radiation Physics, Department of Physics, NOVA School of Science and Technology, Caparica, Portugal
Biography: Helena Cristina Vasconcelos is an Associate Professor at the Faculty of Science and Technology of Azores University. She is a research member of the Laboratory for Instrumentation, Biomedical Engineering and Radiation Physics (LIBPhys). She has received her Bachelor’s degree in Physics and Materials Engineering in 1990 from NOVA University of Lisbon, obtaining, in 1999, the PhD in Materials Engineering from Instituto Superior Técnico, Lisbon. Her main research interests are in optical materials, fluorescence, and photonics (rare-earth doped glasses). Other interests include the development of materials for commercial use in solid targets to produce radioisotopes in low/medium energy cyclotrons.

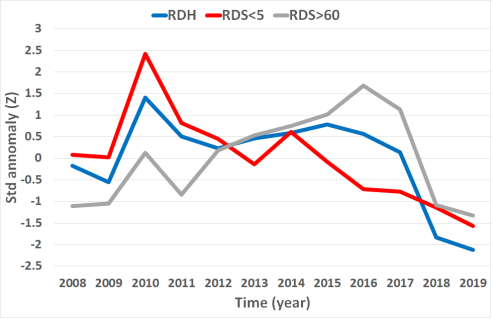
Figure 1. Normalized series of the average annual number of admissions with respiratory diseases in the Hospital da Horta, for the period from 2008 to 2019.
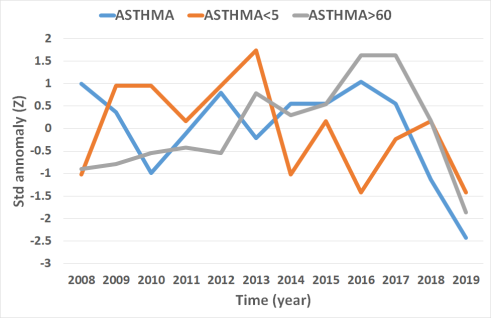
Figure 2. Normalized series of the average annual number of admissions with asthma in the Hospital da Horta, for the period from 2008 to 2019.
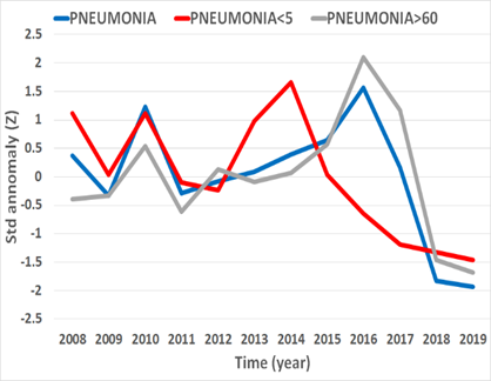
Figure 3. Normalized series of the annual average number of hospitalizations with pneumonia in the Hospital da Horta, for the period 2008.
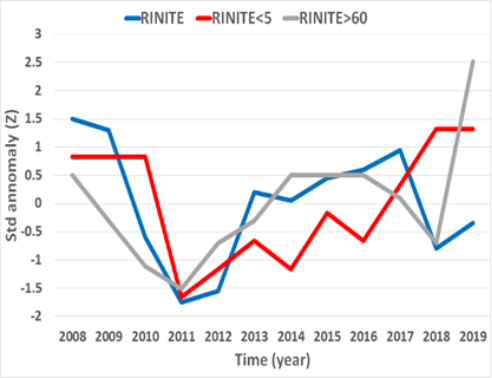
Figure 4. Normalized series of the annual average number of hospitalizations with rhinitis in the Hospital da Horta, for the period 2008.
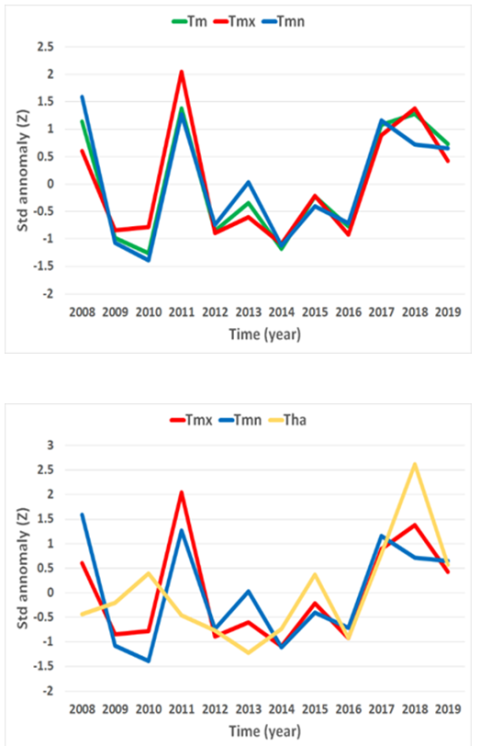
Figure 5. Normalized series of annual averages of mean (Tm), maximum (Tmx) and minimum (Tmn) daily temperatures (up) and daily thermal amplitude (Tha) (down) observed at the meteorological station of Príncipe Alberto do Monaco Observatory (Horta), for the period 2008 to 2019.
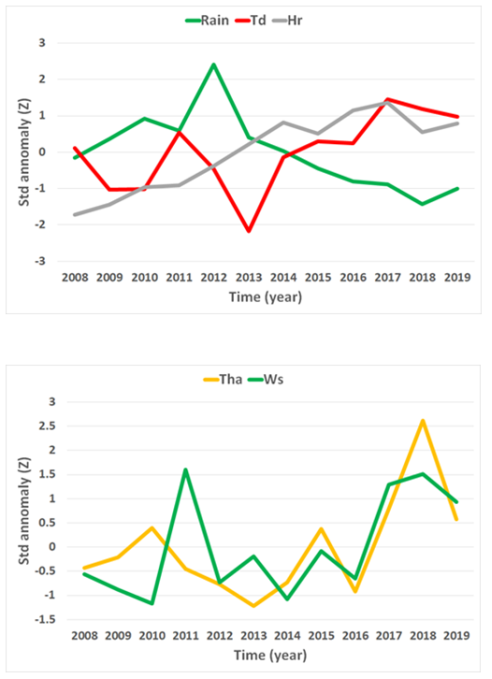
Figure 6. Normalized series of annual averages of daily total precipitation (Rain), daily averages of relative humidity (Hr) and dew point (Td) (up), as well as daily temperature amplitude (Tha) and mean wind speed (Ws) (down) observed at the meteorological station of Príncipe Alberto do Monaco Observatory (Horta), for the period 2008 to 2019.
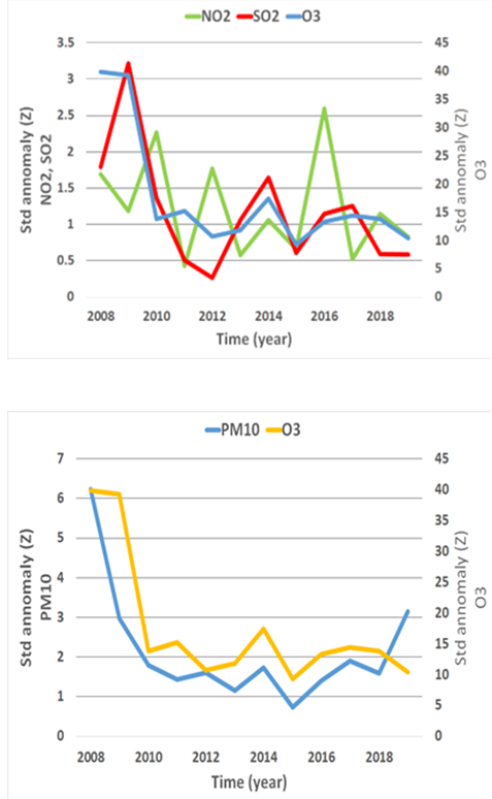
Figure 7. Normalized series of annual averages of concentrations of nitrogen dioxide (NO2), sulphur di-oxide (SO2) (up), particulate matter (PM10) and ozone (O3) (down), observed at the Espalhafatos air quality station (Faial), for the period 2008 to 2019.
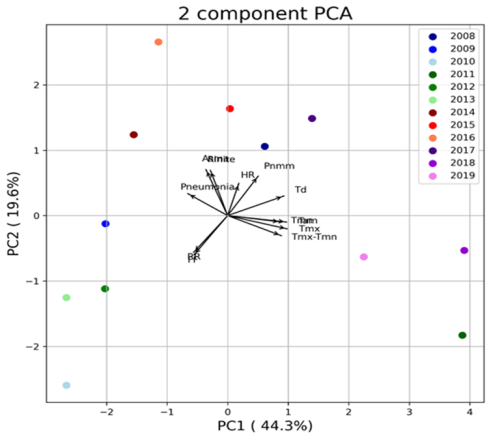
Figure 8. Graphical representation of the first two principal components for the set of meteorological variables and for the diseases under study, for the years 2008 to 2019.
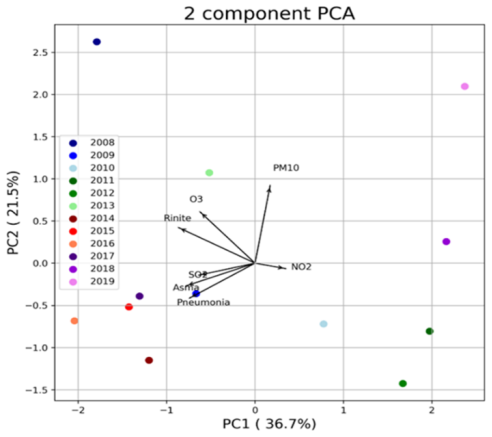
Figure 9. Graphical representation of the first two principal components for the set of air quality variables and for the diseases under study, for the years 2008 to 2019.
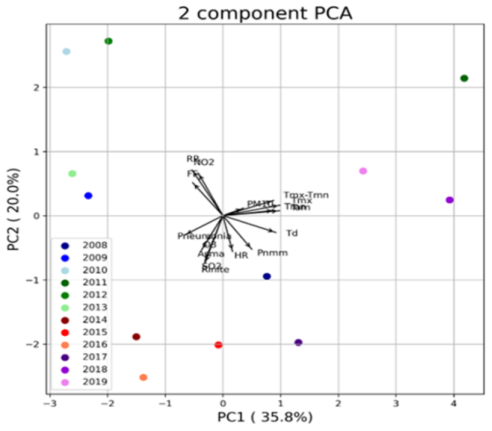
Figure 10. Graphical representation of the first two principal components for the set of variables under study, for the years 2008 to 2019.

